A Scientific Explanation For Why There Are So Many IV, Blood Draw, Injection of Contrast And Blood Donation Failures
By
M. Gail Stotler, Vein Access Technologist / B.S.N., R.N. / B.A. Biology
________________________________________________________________________________________________
By
M. Gail Stotler, Vein Access Technologist / B.S.N., R.N. / B.A. Biology
________________________________________________________________________________________________
Abstract In 2008, there were 37.5 million hospital admissions in the United States. Every hospital patient gets at least one blood draw on admission, 7 out of 10 get an IV, and 3 out of 10 get an injection of contrast totaling a minimum of 263 million vein access procedures in hospitals alone. At least 4 out of every 10 sticks fail, and not just once. That calculates out to an estimated 174 million vein access failures divided between the IV, the blood draw, and the injection of contrast. Why so many failures? The primary explanation is that the current methods of vein access are not science based; they are anecdotally and empirically based and rooted in the 19th century.
According to history, two thousand or more years ago bloodletting began, the first form of vein access. And in the 5th-19th centuries, when it was most popular, that primitive form of vein access involved the use of a scalpel and a tourniquet and other primitive devices.(1,2) Was the tourniquet used to promote venous distention, to bleed more; was it used to prevent the venous blood flow from going up, so more would go out (the ‘damming’ effect’): or was it used because they feared that bleeding to death could actually occur and the tourniquet was used in its truest sense – to stop bleeding? Only vague written descriptions of the practice exist and only a general description of the thought process behind the practice can be found. But considering the absence of scientific information about the body at that time, using the tourniquet to prevent bleeding to death is the logical answer.
But what we do know for sure is that 2000 years ago, when vein access began, the medical community did not have the knowledge about anatomy and physiology, or the tool technology that we have now. We also know that in the 5th -19th centuries it was primarily a barber who did blood letting. Barbers were not scientists, nor were they science educated. So the foundation for vein access, laid in those days, was not based upon science.
And , in spite of the advances in the tools that have been made over the last 200 years, like the hypodermic needle and its use to enter a vein, and the vacutainer system in 1949 that sucks blood into the tube for diagnostic blood draws, and other advances in tool technology, the actual procedure of locating and accessing the vein has not changed (much); they still smack, slap, flick and tap the vein and they still use the tourniquet.
The vein access procedure of today was built on that 5th-19th century non-scientific foundation. And that is why there are so many vein access failures.
This article will describe and debunk just a few of the well established anecdotal and empirical practices of this old procedure. There are too many to identify all of them here.
According to history, two thousand or more years ago bloodletting began, the first form of vein access. And in the 5th-19th centuries, when it was most popular, that primitive form of vein access involved the use of a scalpel and a tourniquet and other primitive devices.(1,2) Was the tourniquet used to promote venous distention, to bleed more; was it used to prevent the venous blood flow from going up, so more would go out (the ‘damming’ effect’): or was it used because they feared that bleeding to death could actually occur and the tourniquet was used in its truest sense – to stop bleeding? Only vague written descriptions of the practice exist and only a general description of the thought process behind the practice can be found. But considering the absence of scientific information about the body at that time, using the tourniquet to prevent bleeding to death is the logical answer.
But what we do know for sure is that 2000 years ago, when vein access began, the medical community did not have the knowledge about anatomy and physiology, or the tool technology that we have now. We also know that in the 5th -19th centuries it was primarily a barber who did blood letting. Barbers were not scientists, nor were they science educated. So the foundation for vein access, laid in those days, was not based upon science.
And , in spite of the advances in the tools that have been made over the last 200 years, like the hypodermic needle and its use to enter a vein, and the vacutainer system in 1949 that sucks blood into the tube for diagnostic blood draws, and other advances in tool technology, the actual procedure of locating and accessing the vein has not changed (much); they still smack, slap, flick and tap the vein and they still use the tourniquet.
The vein access procedure of today was built on that 5th-19th century non-scientific foundation. And that is why there are so many vein access failures.
This article will describe and debunk just a few of the well established anecdotal and empirical practices of this old procedure. There are too many to identify all of them here.
_____________________________________________________________________________________________________________________________________
As mentioned in the opening statement, in 2008, in the U.S. hospitals alone, there were over 174 million vein access failures, and that doesn’t even begin to describe all of the collateral damage and affected medical outcomes associated with these failures. But how did we arrive at that failure number?
Calculations used to arrive at this number, were based upon these factors:
The following estimated numbers for these vein access procedures was based upon a 5.5 average hospital LOS and typical ordering frequency of these procedures.
Every patient gets a blood draw on admission and usually daily for the LOS. 37 million x 5.5 LOS days = 203 million blood draws
Five out of every 10 patients get an IV on admission and at least one required IV change during that 5.5 LOS (and not factoring in the IV changes due to IV infiltrations
which has an approximate 50% occurrence rate). 37 million x 0.5 x 2 during LOS = 36 million IVs
Three out of every 10 patients get an injection of contrast for an x-ray procedure on admission and one more during that 5.5 day LOS.
37 million x 0.33 x 2 = 24 million injections of contrast
Giving us a total of: 203 + 36 + 24 = 263 million vein accesses in 2008 (min.) Now we need to factor in the industry recognized failure rate.
The industry acknowledges a failure rate experience of 30-40% with vein access procedures in the three disciplines; nursing, laboratory medicine and radiology.
With a 40% failure rate for each stick, and an industry accepted limit of up to 6 sticks per procedure, if need be, these are the numbers:
1st stick attempt failures – 263 million x 0.40 = 105 million failures
2nd stick attempt failures – 105 million x 0.40 = 42 million failures
3rd stick attempt failures – 42 million x 0.40 = 16.8 million failures
4th stick attempt failures - 16.8 million x 0.40 = 6.7 million failure
5th stick attempt failures – 6.7 million x 0.40 = 2.7 million failures
6th stick attempt failures - 2.7 million x 0.40 = 1 million failures ….and, at this point, they usually go and get a ‘sure sticker’….
The total number of vein access failure for those 263 million ordered procedures is: 174 million vein access failures.
____________________________________________________________________________________________________________________________________
As mentioned in the opening statement, in 2008, in the U.S. hospitals alone, there were over 174 million vein access failures, and that doesn’t even begin to describe all of the collateral damage and affected medical outcomes associated with these failures. But how did we arrive at that failure number?
Calculations used to arrive at this number, were based upon these factors:
- The AHA’s reported statistics for hospital admissions in 2008 of 37 million.3
- AHA’s calculated number of hospital days for 2008 - 200 million hospital days.(3)
- CDC reported statistics that the LOS for 2008 - 5.5 days (4)
The following estimated numbers for these vein access procedures was based upon a 5.5 average hospital LOS and typical ordering frequency of these procedures.
Every patient gets a blood draw on admission and usually daily for the LOS. 37 million x 5.5 LOS days = 203 million blood draws
Five out of every 10 patients get an IV on admission and at least one required IV change during that 5.5 LOS (and not factoring in the IV changes due to IV infiltrations
which has an approximate 50% occurrence rate). 37 million x 0.5 x 2 during LOS = 36 million IVs
Three out of every 10 patients get an injection of contrast for an x-ray procedure on admission and one more during that 5.5 day LOS.
37 million x 0.33 x 2 = 24 million injections of contrast
Giving us a total of: 203 + 36 + 24 = 263 million vein accesses in 2008 (min.) Now we need to factor in the industry recognized failure rate.
The industry acknowledges a failure rate experience of 30-40% with vein access procedures in the three disciplines; nursing, laboratory medicine and radiology.
With a 40% failure rate for each stick, and an industry accepted limit of up to 6 sticks per procedure, if need be, these are the numbers:
1st stick attempt failures – 263 million x 0.40 = 105 million failures
2nd stick attempt failures – 105 million x 0.40 = 42 million failures
3rd stick attempt failures – 42 million x 0.40 = 16.8 million failures
4th stick attempt failures - 16.8 million x 0.40 = 6.7 million failure
5th stick attempt failures – 6.7 million x 0.40 = 2.7 million failures
6th stick attempt failures - 2.7 million x 0.40 = 1 million failures ….and, at this point, they usually go and get a ‘sure sticker’….
The total number of vein access failure for those 263 million ordered procedures is: 174 million vein access failures.
____________________________________________________________________________________________________________________________________
Why has this information gone undetected, unnoticed, not gathered and not reported for all of these years? There are many explanations for this as well.
_____________________________________________________________________________________________________________________________________
- The medical industry does not track vein access failures – individually for each discipline or as the same common problem for all three disciplines. Therefore, they don’t see the ‘174 million’ global picture.
- Each discipline, nursing, lab and x-ray, struggles with vein access, but that’s what they see it as - a ‘struggle’ - but not a problem. (One little caveat – in 2009, one of the leading laboratory tool manufacturers in the world did a world wide survey to identify the #1 laboratory problem with blood diagnostics – vein access was unequivocally ranked the #1 problem).
- Each discipline sees THEIR vein access issue as independent and not related to the other disciplines- because the procedural mission is different.
- Hospital administrations, when approached with this issue, pass the responsibility on to their departments heads – it’s not viewed as an administrative problem. And the department heads aren’t in position to make standards of care changes.
- Teaching institutions just teach what they have always taught for the last 200+ years – the old methods.
- The people who teach this skill and the people who do this skill have a minimal science education. A&P taught at the allied health level is minimal compared to graduate and medical school level. And they are ‘missing’ some very important A&P information. And the PhDs who teach in some of these programs are not teaching the higher level of A&P and, more importantly, do not apply this science to the skill - because they ‘don’t do vein access’. And besides advanced A&P, there is physics, chemistry and math that is also missing from their education and training.
- The one medical professional who has enough science education to potentially identify this problem and solve this problem is the physician – but the primary care provider doesn’t do vein access – not usually. So it’s not on their radar.
_____________________________________________________________________________________________________________________________________
Fact #1 - Gray's Anatomy of the Vein Fact #3 Needle Angle of Entry

Let’s consider just a few here. This will clearly demonstrate the ‘missing’ science in the current vein access procedures and clearly demonstrate the impact that this has on the procedure. This information cannot be found in any of the current training programs or in any written descriptions in books or teaching manuals on the skill of vein access for blood draws, IVs or injection of contrast, except one.
Consider these facts:
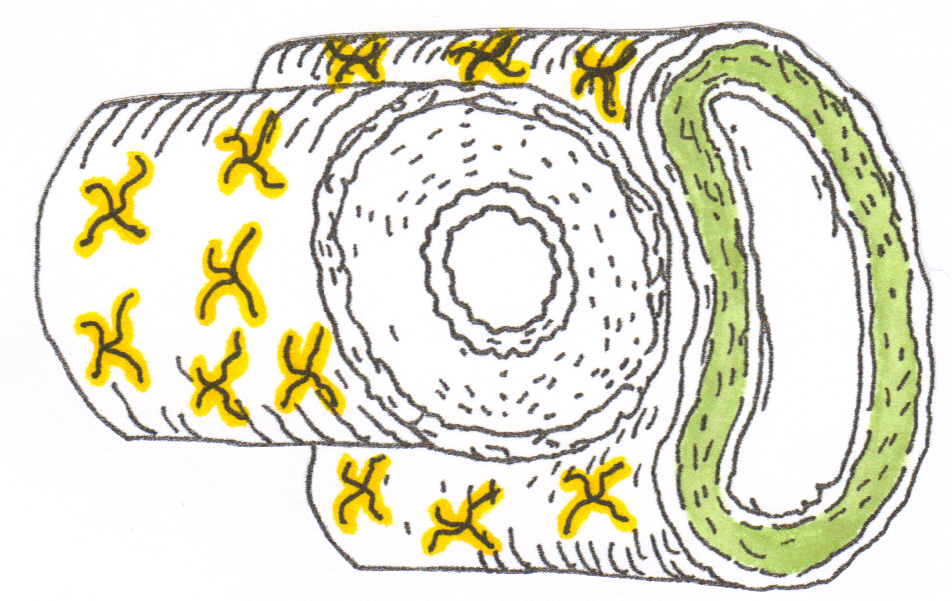
#1 Gray’s Anatomy tells us that the vein wall is innervated AND has a middle layer of smooth muscle.(6) Guyton’s Physiology tells us that negative stimuli
to the nerve tells that muscle to contract.(7)
PROBLEM: If you smack, slap, flick or tap that vein, in an effort to ‘raise the vein’, in an effort to locate it, you will cause vaso-Constriction.
#2 A natural dilatation, with heat or gentle touch, of the adult vein results in an average 2 mm diameter dilatation of that vein. Article: Van Bemmelen, Kelly
and Biebea, Journal of Vascular Surgery, Volume 42, Issue 5, Pg. 957-962 (November 2005), Improvement in the visualization of superficial arm veins
being evaluated for access and bypass.8 This study used heat to achieve a neuromuscular dilatation – oddly enough, the same method that Dr. Burke used
in his.
An artificial dilatation, from applying a tight tourniquet, causes an over distention of that vein greater than 2 mm. To our knowledge, no studies have been done to
document the average size of distention with a tight tourniquet, but palpation alone will clearly demonstrate the size of the vein over distention with the use
of the tourniquet compared to the naturally dilated vein with the new palpation technique by Vein Access Technologies (without the use of the tourniquet).
PROBLEM: There is an anatomical limit to how much the vein wall’ nerves and smooth muscle can be stretched before injury occurs to those tissues and that
segment of vein wall. (injury i.e. varicosity, infiltration, vein rupture).
#3 A <30 degree angle of entry of the needle through the vein wall results in a vein wall injury 4-5 times the size that a >45 degree angle of entry causes.10
PROBLEM: Injury size is extended. Pain is maximized. Clotting time will be extended. Healing time will be extended. The likelihood of bruising is greater.
____________________________________________________________________________________________________________________________________
Consider these facts:
#1 Gray’s Anatomy tells us that the vein wall is innervated AND has a middle layer of smooth muscle.(6) Guyton’s Physiology tells us that negative stimuli
to the nerve tells that muscle to contract.(7)
PROBLEM: If you smack, slap, flick or tap that vein, in an effort to ‘raise the vein’, in an effort to locate it, you will cause vaso-Constriction.
#2 A natural dilatation, with heat or gentle touch, of the adult vein results in an average 2 mm diameter dilatation of that vein. Article: Van Bemmelen, Kelly
and Biebea, Journal of Vascular Surgery, Volume 42, Issue 5, Pg. 957-962 (November 2005), Improvement in the visualization of superficial arm veins
being evaluated for access and bypass.8 This study used heat to achieve a neuromuscular dilatation – oddly enough, the same method that Dr. Burke used
in his.
An artificial dilatation, from applying a tight tourniquet, causes an over distention of that vein greater than 2 mm. To our knowledge, no studies have been done to
document the average size of distention with a tight tourniquet, but palpation alone will clearly demonstrate the size of the vein over distention with the use
of the tourniquet compared to the naturally dilated vein with the new palpation technique by Vein Access Technologies (without the use of the tourniquet).
PROBLEM: There is an anatomical limit to how much the vein wall’ nerves and smooth muscle can be stretched before injury occurs to those tissues and that
segment of vein wall. (injury i.e. varicosity, infiltration, vein rupture).
#3 A <30 degree angle of entry of the needle through the vein wall results in a vein wall injury 4-5 times the size that a >45 degree angle of entry causes.10
PROBLEM: Injury size is extended. Pain is maximized. Clotting time will be extended. Healing time will be extended. The likelihood of bruising is greater.
____________________________________________________________________________________________________________________________________
This level of science and the application of the science to the skill is what is missing from the current training programs and teaching manuals, and explains the vein access difficulties and the vein access failures.
How did this happen and how does it continue to happen? Let’s turn to the profession’s frequently employed use of the term ‘evidence-based’ for an explanation, because
when the industry is approached today with any new information they immediately want to know “Is this information ‘evidence based?”, holding up that vernacular as if it were a shield protecting their old method and defending against the invasion of the new.
The definition of “evidence based” states that the evidence be based upon a ‘scientific method’ before it can be applied to clinical decision making.9 The foundation, then, of Evidence-based medicine (EBM) or Evidence-based practice (EBP) is science. The evidentiary clinical outcome of that science applied to the clinical practice is the second part of the process. It’s a combination of science and evidence. But science is the foundation. And the original and current methods of vein access are not science based (and their evidence demonstrates a 40% failure rate).
The term Evidence-based treatment (EBT) or empirically-supported treatment (EST)9 more accurately describes how the current vein access got started and why it continues to this day. Recall the beginning of this article. Phlebotomy, the first form of vein access, is 2000 years old and the originators of the current ‘tourniquet technique’ vein access were the 5th-19th century barbers.
….Many areas of professional practice, such as medicine…., have had periods in their pasts where practice was based on loose bodies of knowledge.
Some of the knowledge was simply lore that drew upon the experiences of generations of practitioners, and much of it had no truly scientific evidence on
which to justify various practices…… Wikipedia (9)
It is this author’s opinion that the vein access procedure of today is one of those ‘loose bodies of knowledge’; it is based upon anecdotal and empirical experience, not science.
The current vein access techniques may be old and well established (meeting some of that criteria for ‘evidence-based’), and ingrained in the brains of millions of people around the world, and written in hundreds, if not thousands, of books, but the evidence of millions of vein access failures warrants investigation.
_____________________________________________________________________________________________________________________________________
How did this happen and how does it continue to happen? Let’s turn to the profession’s frequently employed use of the term ‘evidence-based’ for an explanation, because
when the industry is approached today with any new information they immediately want to know “Is this information ‘evidence based?”, holding up that vernacular as if it were a shield protecting their old method and defending against the invasion of the new.
The definition of “evidence based” states that the evidence be based upon a ‘scientific method’ before it can be applied to clinical decision making.9 The foundation, then, of Evidence-based medicine (EBM) or Evidence-based practice (EBP) is science. The evidentiary clinical outcome of that science applied to the clinical practice is the second part of the process. It’s a combination of science and evidence. But science is the foundation. And the original and current methods of vein access are not science based (and their evidence demonstrates a 40% failure rate).
The term Evidence-based treatment (EBT) or empirically-supported treatment (EST)9 more accurately describes how the current vein access got started and why it continues to this day. Recall the beginning of this article. Phlebotomy, the first form of vein access, is 2000 years old and the originators of the current ‘tourniquet technique’ vein access were the 5th-19th century barbers.
….Many areas of professional practice, such as medicine…., have had periods in their pasts where practice was based on loose bodies of knowledge.
Some of the knowledge was simply lore that drew upon the experiences of generations of practitioners, and much of it had no truly scientific evidence on
which to justify various practices…… Wikipedia (9)
It is this author’s opinion that the vein access procedure of today is one of those ‘loose bodies of knowledge’; it is based upon anecdotal and empirical experience, not science.
The current vein access techniques may be old and well established (meeting some of that criteria for ‘evidence-based’), and ingrained in the brains of millions of people around the world, and written in hundreds, if not thousands, of books, but the evidence of millions of vein access failures warrants investigation.
_____________________________________________________________________________________________________________________________________
Bibliography Page
1. The History of Phlebotomy, http://www.mtn.org/quack/devices/phlebo.htm.
2. History of Bloodletting by Phlebotomy, Liakat Ali Parapia, 2008-09-06 Medline Article.
3. http://www.aha.org/aha/resource-center/Statistics-and-Studies/fast-facts.html American Hospital Association, Resource Center, Fast Facts
4. http://www.cdc.gov/nchs/fastats/hospital.htm CDC and Prevention, Fast Stats
5. Care and Feeding of Veins, Dr. Erwin L Burke, NEJM, June 4, 1970 issue, pg. 1336-1327.
6. Gray’s Anatomy, 13th edition, pg. 1131
7. Guyton and Hall’s, Textbook of Medical Physiology.
8. Van Bemmelen, Kelly and Biebea, Journal of Vascular Surgery, Volume 42, Issue 5, Pg. 957-962 (November 2005), Improvement in the visualization of superficial arm vei2005), Improvement in the visualization of superficial arm veins being evaluated for access and bypass.
9. Wikipedia, definition of ‘evidence based’.
10. The Science Behind the Skill of Vein Access, M. Gail Stotler, 2006
1. The History of Phlebotomy, http://www.mtn.org/quack/devices/phlebo.htm.
2. History of Bloodletting by Phlebotomy, Liakat Ali Parapia, 2008-09-06 Medline Article.
3. http://www.aha.org/aha/resource-center/Statistics-and-Studies/fast-facts.html American Hospital Association, Resource Center, Fast Facts
4. http://www.cdc.gov/nchs/fastats/hospital.htm CDC and Prevention, Fast Stats
5. Care and Feeding of Veins, Dr. Erwin L Burke, NEJM, June 4, 1970 issue, pg. 1336-1327.
6. Gray’s Anatomy, 13th edition, pg. 1131
7. Guyton and Hall’s, Textbook of Medical Physiology.
8. Van Bemmelen, Kelly and Biebea, Journal of Vascular Surgery, Volume 42, Issue 5, Pg. 957-962 (November 2005), Improvement in the visualization of superficial arm vei2005), Improvement in the visualization of superficial arm veins being evaluated for access and bypass.
9. Wikipedia, definition of ‘evidence based’.
10. The Science Behind the Skill of Vein Access, M. Gail Stotler, 2006
Published by
Vein Access Technologies, a division of The Nurses’ Station, P.C.
#2 Terminal Drive, Suite 1, East Alton, Illinois 62024
618-259-778I
www.veinaccesstechnologies.com
Copyright © 2007-2014. All rights reserved
Vein Access Technologies, a division of The Nurses’ Station, P.C.
#2 Terminal Drive, Suite 1, East Alton, Illinois 62024
618-259-778I
www.veinaccesstechnologies.com
Copyright © 2007-2014. All rights reserved